Glycyrrhizic acid as a drug candidate for COVID-19
Therapies to counteract the damage caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) have been few and far between, despite efforts to discover new drugs and repurpose already approved drugs that may target the viral proteins.
Without effective therapeutics, clinicians have extended their search into areas of plant-derived compounds. Traditional Chinese medicine (TCM), for example, has yielded several effective compounds against the earlier SARS-CoV and is currently part of the treatment approach of the coronavirus disease 20198 (COVID-19) in China.
Background
The swift development of COVID-19 vaccines and their subsequent rollout in many parts of the world has made considerable progress in reducing the number and severity of COVID-19 cases. Despite their utility, the emergence of new SARS-CoV-2 variants that are less susceptible to neutralizing antibodies (nAbs) elicited by the parental Wuhan strain has challenged the success of these vaccines.
In addition to challenging the efficacy of current vaccines, many of these new SARS-CoV-2 strains are also more transmissible than the wild-type SARS-CoV-2 strain. As a result, there has been a significant rise in COVID-19 infections in many areas around the world, particularly those which have yet to vaccinate a majority of their populations.
In the current study, which was published in Frontiers in Pharmacology, the researchers focused on licorice, which has the active compound glycyrrhizic acid (GA). GA has been found to have antiviral activity, particularly against SARS-CoV-2.
GA benefits in COVID-19
In the current study, GA was found to have both protein-targeting properties and immunomodulatory properties. It also has synergistic activity with many drugs that enhanced its antiviral potential against SARS-CoV-2. This indicates the potential role of GA as a COVID-19 therapy.
In severe and critical COVID-19, the cytokine storm has been well documented and is associated with an increased risk of multi-organ dysfunction or failure, coupled with acute respiratory distress syndrome, and death. In the clinical setting, the potent anti-inflammatory drug dexamethasone, which is a corticosteroid, has been found to improve survival outcomes in this group of COVID-19 patients.
TCM has been widely used in the SARS outbreak of 2002, with claims that it has reduced the mortality rate when used along with Western medicine. Among the most commonly used herbal medicines in TCM is licorice, which is known to have antiviral and antibacterial properties.
GA has been shown in silico to bind to many key SARS-CoV-2 proteins, including the spike, receptor-binding domain, ribonucleic acid (RNA) polymerase, as well as to the angiotensin-converting enzyme 2 (ACE2) receptor, which is the host cell receptor that SARS-CoV-2 binds to when entering cells.
GA and the immune response
The current study shows that GA is an adjuvant to immune activation, and thus enhances the immune antiviral response while the virus is in the incubation period. GA also mutes the cytokine storm caused by SARS-CoV-2, while modulating viral invasion via its effect on steroid metabolism.
In view of its synergistic effect on SARS-CoV-2, GA might reduce the mortality rate of COVID-19. However, further studies are needed to explore its utility as an adjuvant in treating this condition.
SARS-CoV-2 activates CD4+ T-lymphocytes after entering the host cell; however, it also triggers several immune escape mechanisms. This, coupled with the delayed adaptive immune response and the long period required to clear the virus, causes lymphopenia. By promoting T-cell proliferation and by virtue of its adjuvant activity on T-helper type 1 (Th1) cells, GA increases the immune response to SARS-CoV-2.
Secondly, GA causes infected host cells that contain the latent virus to undergo apoptosis, which could help prevent the further spread of the virus.
The Th1-secreted cytokine called granulocyte-macrophage colony-stimulating factor (GM-CSF) is implicated in the release of inflammatory factors and the rapid onset of pneumonia. This involves the expression of interleukin 6 (IL-6), perhaps by the hyper-activation of nuclear factor-κB (NF-κB), which induces a vicious cascade of inflammatory mediator release.
SARS-CoV-2 may bind to lipopolysaccharide (LPS) antigens, further intensifying this NF-κB response, and thus leading to the cytokine storm and ARDS. By inhibiting NF-κB expression, GA could prevent hyper-inflammatory phenomena in COVID-19.
GA can also bind to high mobility group box-1 (HMGB1), which is a biomarker that is associated with acute lung injury (ALI) characteristically seen in severe COVID-19, as well as of severe systemic inflammation. HMGB1 reduces the antimicrobial response of the body and thus increases the risk of death, as well as promotes SARS-CoV-2 invasion and replication. Thus, GA can disrupt these damaging pathways as well, thereby preventing inflammation and ARDS.
GA and COVID-19 comorbidities
Diabetes is a risk factor for severe COVID-19, as it promotes cholesterol uptake into lipid rafts, or cell membrane microdomains rich in lipids. These rafts are attachment points for the virus, thus promoting viral entry into the host cells. GA appears to reduce the invasion of SARS-CoV-2 by reducing lipid raft size.
Cholesterol builds up within the endothelium in hypertension and hypercholesterolemia, which can promote blood clots. Cholesterol also drives platelet aggregation and clot formation.
GA can reduce the cholesterol domain size on the endothelial cell membrane, thus inhibiting these effects. Since GA may cause pseudoaldosteronism and hypertension following its long-term use, spironolactone may be required in these patients.
In metabolic syndrome, a clinical constellation comprising obesity, hyperglycemia, hypertension, and dyslipidemia, the risk of severe COVID-19 and ARDS is high, while LPS levels in the blood are increased. Thus, GA may play a major role in preventing this deterioration.
GA and inflammation
GA also inhibits tumor necrosis factor (TNF)-α, which may prevent severe intestinal inflammation in patients with COVID-19 and irritable bowel syndrome. Further, GA may protect the nervous system through its ability to inhibit apoptosis and HMGB1 activity, which may prevent inflammation and ischemic injury to the brain.
Activating transcription factor 2 (ATF2), which is an inflammatory mediator, mediates the pain associated with inflammation. GA appears to inhibit ATF2 downstream of its activity on P38, thus modulating the pain associated with COVID-19.
GA and steroids
GA can reduce steroid metabolism, which can increase the plasma steroid level, thus preventing shock, as demonstrated in animal models. Thus, corticosteroids and GA could be a synergistic therapeutic approach for COVID-19.
Protective effect of GA in COVID-19
Diabetics are at higher risk for COVID-19; however, new-onset diabetes occurs in about one in seven COVID-19 patients. Perhaps SARS-CoV-2 causes pancreatic islet damage, with resulting failure of insulin secretion and diabetes. Some of the drugs used to treat this infection can also contribute or cause diabetes as a result of their propensity to cause autoimmune disease to the pancreatic islets.
GA has anti-diabetic activity, which enhances its attractiveness in this condition. Moreover, this compound may upregulate the production of inducible nitric oxide synthase enzyme (iNOS), thus promoting the production of NO. This is important, as NO reduces viral replication and ALI due to inflammation, as well as relaxes the pulmonary blood vessels.
This activity by GA may lead to clearing of extracellular fluid from the lung bed, reduce the resistance in the lung vascular bed, and ultimately mitigate ARDS.
GA also protects the liver, and may thus prevent liver injury from the various drugs used at present to treat COVID-19, making it a valuable addition to such protocols.
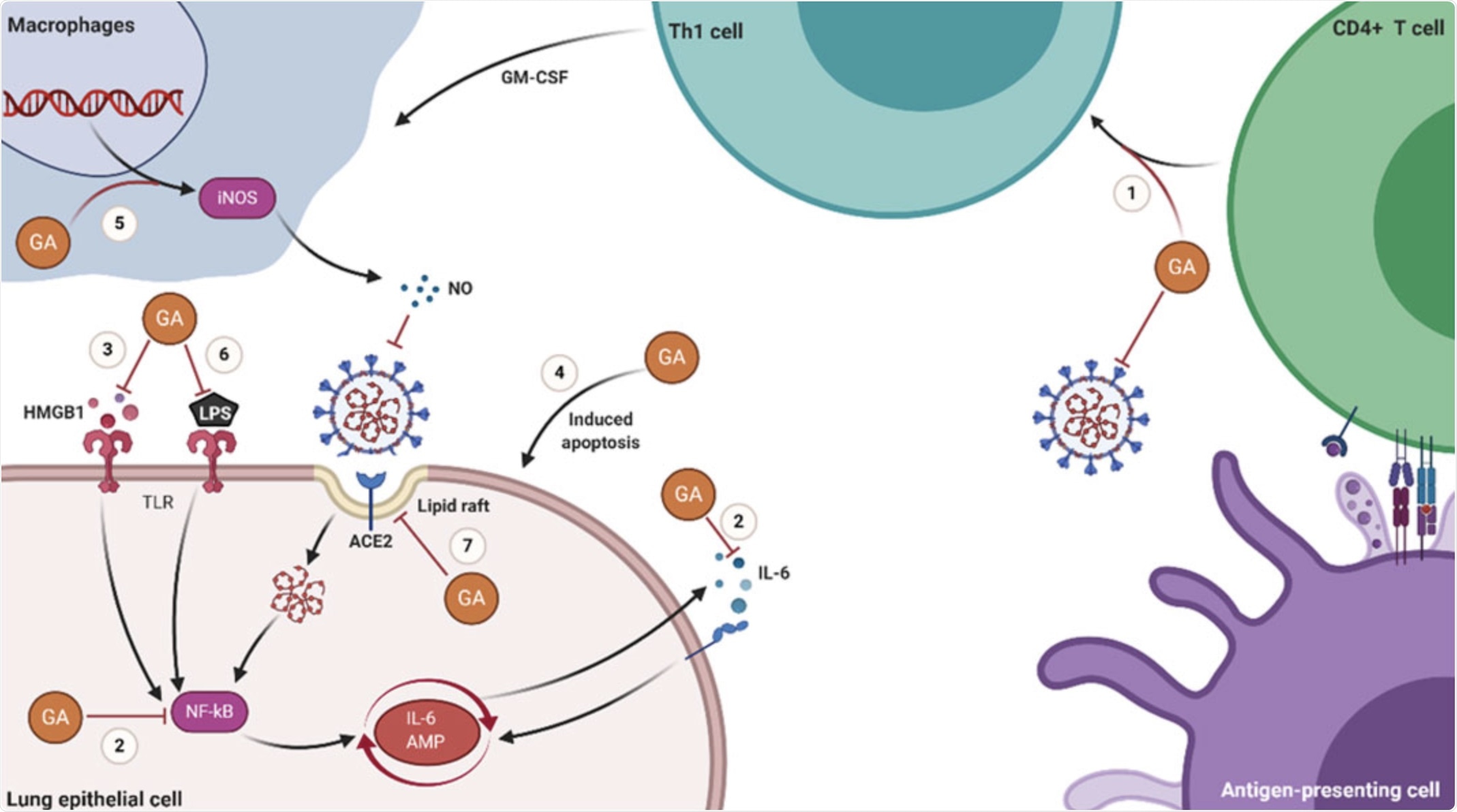 Schematic
diagram of the molecular mechanisms of GA in treating COVID-19. (1) GA
promotes the proliferation of T cells and has Th1 cell immune adjuvant
activity. (2) GA inhibits the production of IL-6 and the activation of
NF-kB. (3) GA inhibits the activity of HMGB1 and the signal transduction
of the HMGB1-TLR4 pathway. (4) GA induces the apoptosis of
host cells latent with SARS-CoV-2. (5) GA stimulates macrophages to
produce NO. (6) GA inhibits the inflammatory response induced by LPS.
(7) GA prevents the invasion of SARS-CoV-2 by reducing the domain of
lipid rafts.
Schematic
diagram of the molecular mechanisms of GA in treating COVID-19. (1) GA
promotes the proliferation of T cells and has Th1 cell immune adjuvant
activity. (2) GA inhibits the production of IL-6 and the activation of
NF-kB. (3) GA inhibits the activity of HMGB1 and the signal transduction
of the HMGB1-TLR4 pathway. (4) GA induces the apoptosis of
host cells latent with SARS-CoV-2. (5) GA stimulates macrophages to
produce NO. (6) GA inhibits the inflammatory response induced by LPS.
(7) GA prevents the invasion of SARS-CoV-2 by reducing the domain of
lipid rafts.
What are the implications?
GA has been used in TCM for a long time as an antiviral and anti-inflammatory compound. Recent research shows its ability to suppress SARS-CoV-2 invasion and replication.
GA appears to bind many SARS-CoV-2 proteins while also having the ability to suppress viral replication. Its ability to assist in the immune response to viruses during the incubation period, dampen the excessive cytokine release, and modulate steroid metabolism make this drug worthy of study in the current attempts to treat COVID-19 more effectively.